How Digital Technology Is Revolutionising Jaw Surgery
Imagine undergoing jaw surgery planned entirely in a three-dimensional virtual environment — where your surgeon rehearses every cut, repositions every bone, and simulates exactly how your face will look afterwards, all before you even step into an operating theatre. This is no longer the future. It is today’s reality for patients undergoing orthognathic surgery at leading centres worldwide.
A 2025 review published in the Australian Dental Journal by Joyce Tin Wing Li and Yiu Yan Leung from The University of Hong Kong provides a comprehensive overview of how digital diagnostics and Virtual Surgical Planning (VSP) are reshaping one of dentistry’s most complex surgical disciplines.
Key Takeaways
|
What Is Orthognathic Surgery?
Orthognathic surgery (OGS) involves the precise repositioning of the jaws to correct a wide spectrum of dentofacial deformities. These range from skeletal malocclusions and facial asymmetries to functional problems such as obstructive sleep apnoea, anterior open bite, and temporomandibular joint disorders. It also plays a vital role in managing complex conditions like cleft lip/palate and craniofacial syndromes.
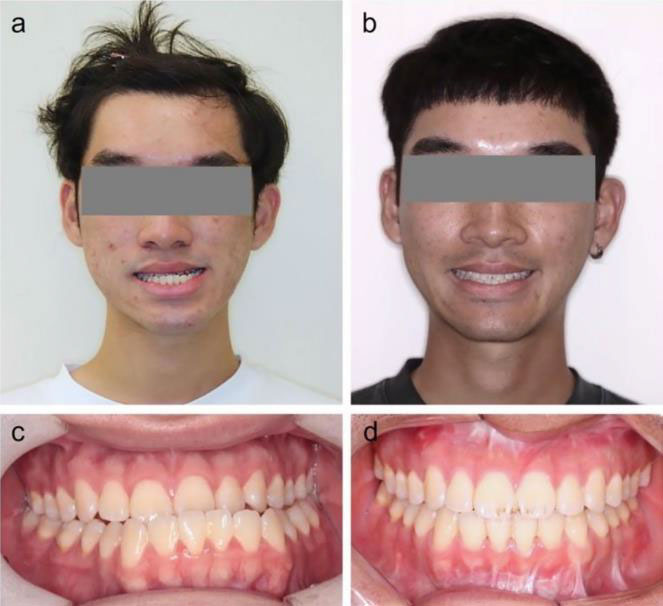
Figure 1 — Preoperative (left) and postoperative (right) clinical photos showing facial and dental changes following orthognathic surgery.
The success of this surgery hinges entirely on meticulous preoperative planning. And for decades, that planning relied on tools that — by today’s standards — were remarkably limited.
The Old Way: Why Traditional Planning Falls Short
Traditional surgical planning (TSP) involved clinical examinations, 2D X-rays (cephalograms), photography, and physical plaster model surgery on an articulator. While this approach served surgeons for generations, it carries several significant limitations:
- Depth perception problems: 2D X-rays cannot fully capture a patient’s complex 3D anatomy. Lateral cephalograms are adequate for sagittal assessment but poorly suited to evaluating asymmetries in the roll and yaw planes.
- Transfer errors: The facebow transfer is particularly prone to misalignment with the Frankfort horizontal plane, introducing errors in the sagittal plane.
- Compounding inaccuracies: The multi-step nature of creating surgical splints from physical models amplifies errors at each stage, potentially compromising final outcomes — especially facial symmetry.
- AI limitations: Current AI-based cephalometric tracing software demonstrates inaccuracies compared to expert human analysis. Clinicians should not rely on these tools alone.

Figure 2 — Traditional plaster model surgery on an articulator. This physical approach is being replaced by fully digital workflows.
Figure 3 — Lateral cephalograms taken for (a) pre-operative diagnosis and (b) post-operative evaluation. These 2D images have inherent depth perception limitations.
The Digital Revolution: Virtual Surgical Planning
VSP replaces the plaster model and 2D radiograph with a fully digital, three-dimensional environment. The workflow integrates several cutting-edge technologies:
1. Cone Beam CT (CBCT)
CBCT provides high-resolution, distortion-free 3D images of bony and dental structures, scanned at less than 1mm slice thickness. This allows surgeons to precisely assess anatomical variations and plan osteotomy paths that avoid critical structures like the descending palatine artery.
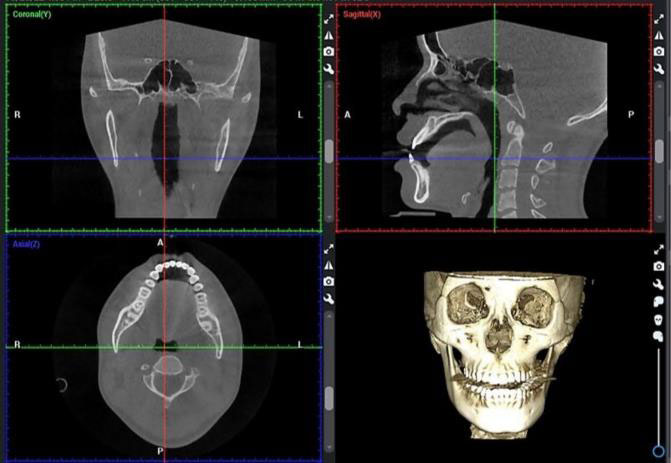
Figure 4 — Cone Beam Computed Tomography (CBCT) showing coronal, sagittal, axial and 3D reconstructed views for pre-operative diagnosis.
2. 3D Facial Scanning
Surface scanners capture precise external facial morphology. When combined with CBCT data, they create a complete craniofacial model enabling advanced soft-tissue simulation and more accurate patient communication about expected outcomes.
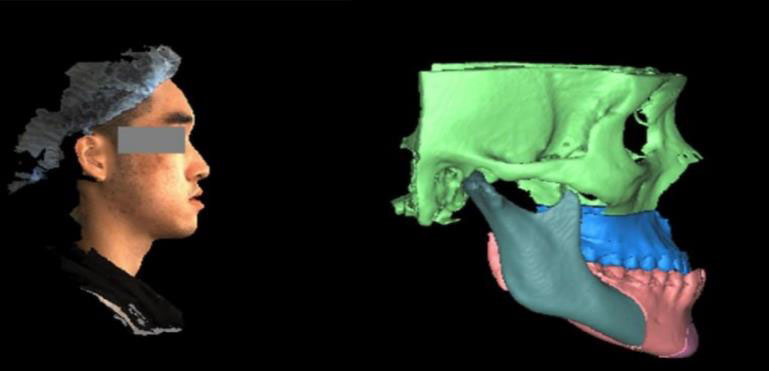
Figure 5 — 3D facial scan overlaid with the digital skeletal model for morphological analysis and surgical simulation.
3. Intra-Oral Scanning
CBCT imaging alone cannot accurately capture dentition detail due to artefacts from orthodontic brackets. Intra-oral scanning fills this gap, feeding directly into 3D surgical planning software without additional processing steps.

Figure 6 — Digital intra-oral scan of dentition, integrated directly into the 3D surgical planning workflow.
Inside the VSP Workflow
The digital workflow is a sequential, integrated process — each step building on the last to create a surgical plan of unprecedented precision.
Step 1: 3D Cephalometric Analysis
CBCT data is imported into specialised software such as ProPlan CMF by Materialise, where a comprehensive 3D cephalometric analysis is performed using 38 identified landmarks. This gives surgeons detailed, objective data on skeletal relationships to guide their planning.
Step 2: Virtual Simulation
VSP software allows surgeons to simulate osteotomies and manipulate a virtual reconstruction of the craniofacial skeleton, visualising bone movements and assessing potential interferences — all before the patient enters the operating room.
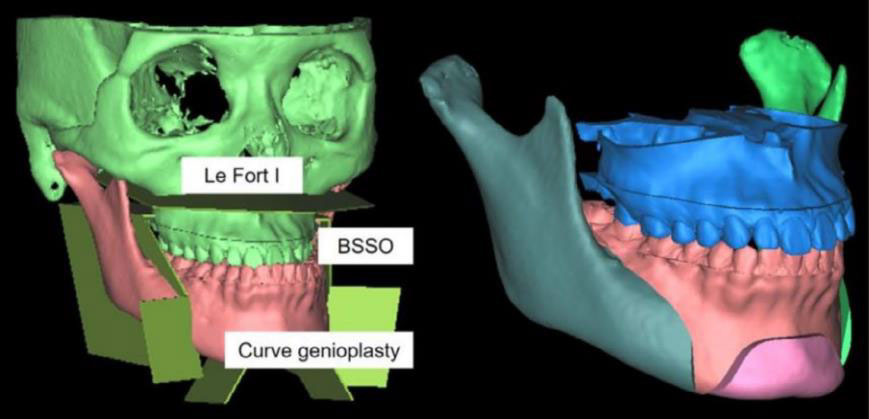
Figure 7 — Virtual surgical planning interface showing simulated Le Fort I osteotomy, bilateral sagittal split osteotomy (BSSO) and genioplasty on the 3D skull model.
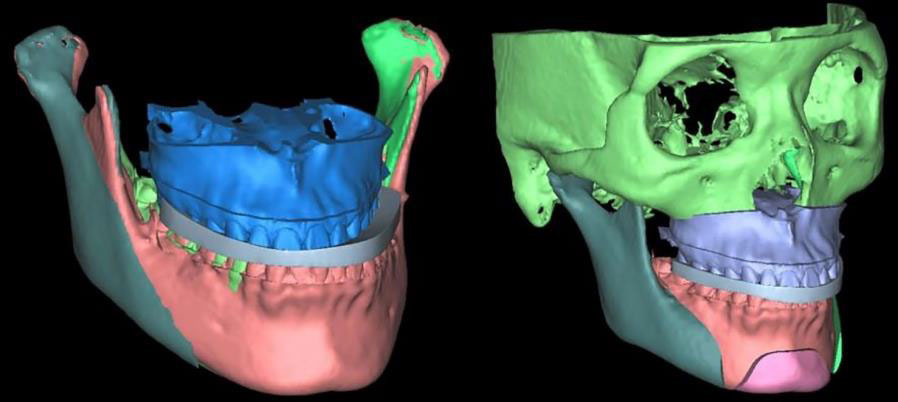
Figure 8 — 3D-printed perioperative and final surgical splints, designed and produced in-house for precise jaw positioning during surgery.
Step 3: Patient-Specific Implants (PSIs)
Perhaps the most remarkable development is the use of patient-specific titanium implants and cutting guides — designed from the patient’s own CBCT data and 3D-printed to precisely match their anatomy. Research shows median deviations of the actual maxilla from planned position in all three axes of less than 1mm.
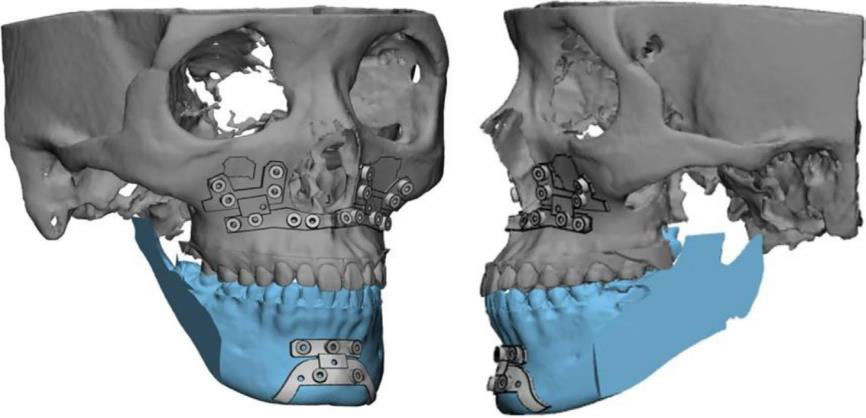
Figure 9 — Computer-aided design of patient-specific fixation plates and cutting guides, modelled precisely on the patient’s bone surface.
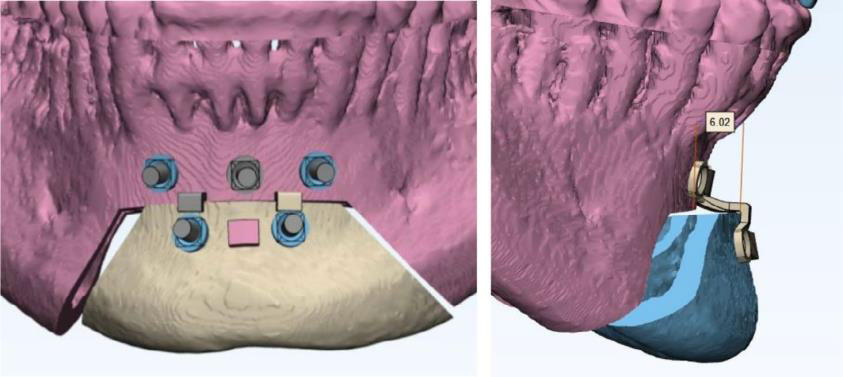
Figure 10 — Virtual design of fixation screws and connection parts, with precise measurements shown for surgical planning.
VSP by the Numbers
|
Clinical Benefits: What This Means for Patients
Meta-analysis data confirms VSP significantly outperforms traditional surgical planning in jaw positioning accuracy. The greatest errors in traditional planning occur in the vertical direction — a challenge that VSP with custom surgical guides substantially reduces.
For patients with obstructive sleep apnoea, CBCT’s large field-of-view enables comprehensive airway visualisation as part of the surgical plan. Digital planning also transforms the patient experience: interactive simulations help patients visualise expected outcomes and set realistic expectations. Studies confirm high satisfaction rates even in complex asymmetric cases, with no revisionary surgery required in full digital planning cohorts.
Challenges and Limitations
Despite its transformative potential, VSP is not without challenges:
- Learning curve and cost: Proficiency in VSP software demands significant training, and initial hardware and software acquisition costs are considerable.
- Intraoperative transfer errors: Errors can occur when seating surgical guides on bony anatomy, meaning final outcomes may still deviate slightly from the virtual plan.
- Soft-tissue prediction limitations: Simulation algorithms are based on average tissue responses and may not fully predict individual healing and aesthetic outcomes.
- Natural Head Position: Accurate NHP transfer to the virtual environment is critical — an error here can skew the entire surgical plan.
What’s Next: The Future of Digital Jaw Surgery
The authors identify several exciting directions for the field:
- Improved soft-tissue prediction algorithms to better anticipate individual aesthetic outcomes
- Augmented reality (AR) intraoperative guidance to overlay the virtual plan directly into the surgical field in real time
- Generative AI for PSI design — automating the creation of patient-specific implants to reduce costs and turnaround times
The Bottom Line
Virtual Surgical Planning represents a genuine paradigm shift in orthognathic surgery. The evidence is compelling: better accuracy, shorter operating times, lower costs, and higher patient satisfaction. For patients facing complex jaw surgery, the adoption of VSP by their surgical team directly influences the precision of outcomes and the quality of their recovery.
For clinicians, the message from Li and Leung is clear: embracing digital workflows is not merely an upgrade — it is becoming the standard of care. As AI, augmented reality, and generative design continue to mature, the boundary between planning and surgery will become increasingly seamless.